Overview
- Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment, though some will become seriously ill and require medical attention.
- Along with growing evidence of neurological symptoms, mental health during the pandemic is a popular topic among researchers, health professionals, policy makers, and the community.
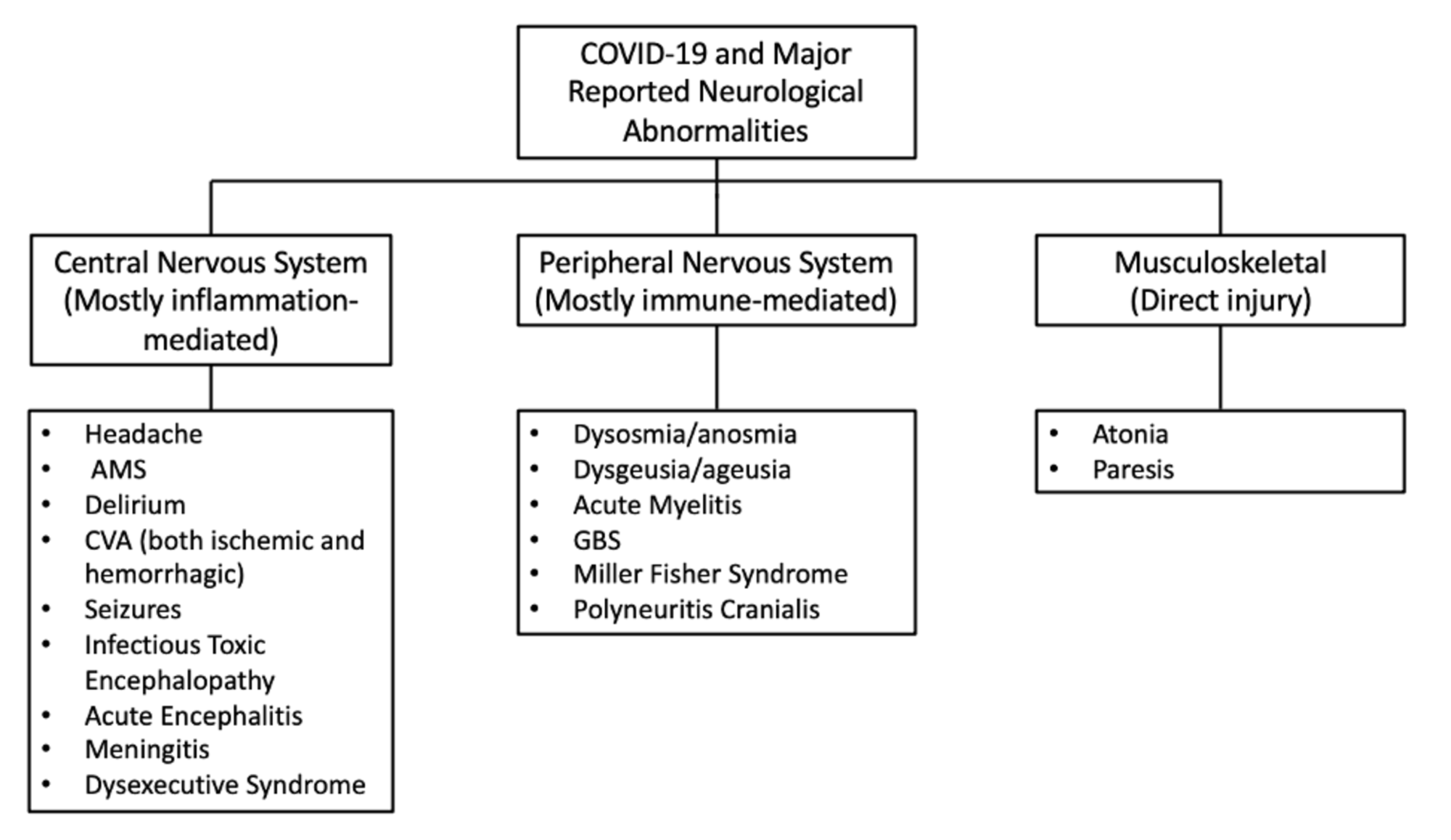
- Some of the neurological symptoms of COVID-19 include confusion, stroke, brain damage, dysexecutive syndrome, olfactory dysfunction, seizures etc. Some of these are a result of an impaired ability of the blood to coagulate properly.
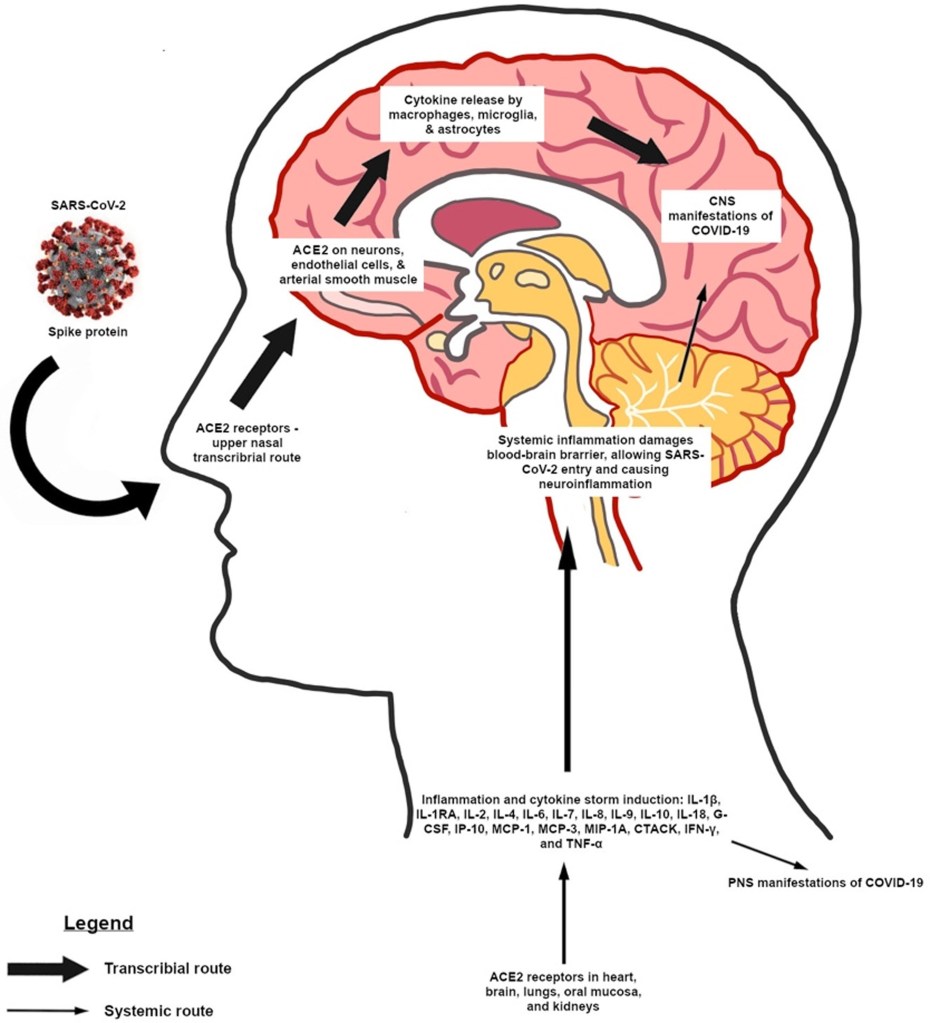
- The virus may enter the central nervous system directly by interacting with specific receptors on neurons in the brainstem, or by inducing systemic inflammation in the body. Some neurological symptoms are a result of too much inflammation.
- The effects of the pandemic and the virus itself are wide-spread on our mental health and include stress, depression, irritability, insomnia, fear, confusion, anger, frustration, boredom etc. Vulnerable groups are affected disproportionately, as a result of weaknesses in the mental healthcare system and other socioeconomic factors.
- Unless addressed robustly and urgently, the impacts of the pandemic will contribute to enormous human suffering, premature mortality, and social breakdown, and will slow down economic recovery.
- Although there was already an enormous crisis relating to mental health before the pandemic, COVID-19 presents a historic opportunity for all countries and global agencies to reassess how human society organizes itself to recover from these impacts.
- Not only should we invest in building mental health systems now but we should also ensure that these investments embrace the diversity of experiences and actions that characterize mental ill health, well beyond the narrow biomedical focus on doctors, diagnoses, and drugs that has dominated mental health policies globally.
This is our third calendar year into the COVID-19 pandemic and I for one am very exhausted, emotionally and physically. Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment, though some will become seriously ill and require medical attention (World Health Organization, 2022). Not only does COVID-19 impact our physical health (which I will describe further below), it has impacted our mental health as well. Uncertain prognoses, severe shortages of resources for testing and treatment, imposition of unfamiliar public health measures (lockdowns and isolations), unemployment and growing financial losses, and conflicting messages from authorities, are among the major stressors that undoubtedly will contribute to widespread emotional distress and increased risk for psychiatric illness associated with COVID-19 (Pfefferbaum & North, 2020). Pandemics may affect the health, safety, and well-being of both individuals and communities, which has the propensity to translate into a range of emotional reactions, unhealthy behaviours, and noncompliance with public health directives in people who contract the disease and in the general population.

In addition to the abovementioned difficulties, the pandemic has undoubtedly had an impact on our social lives, the ways with interact with each other, the way we think and feel, as well as caused or contributed to other more troublesome mental health issues. Along with growing evidence of neurological symptoms, mental health during the pandemic is a popular topic among researchers, health professionals, policy makers, and the community.
I want to shed some light on these two aspects of the current pandemic. Below, I will describe to you how COVID-19 enters the central nervous system, as well as the neurological symptoms of COVID-19. I will then talk about the impacts COVID-19 has had on different aspects of mental health across different populations. Lastly, I have included some points on how we can integrate mental health into disease control efforts.
The Neurological Symptoms of COVID-19
COVID-19 has quickly become a worldwide public health issue typically associated with respiratory symptoms, including fever, shortness of breath, and cough (Pero et al., 2020). However, there is growing evidence that suggests some people who have been infected with COVID-19 may also develop neurologic symptoms including confusion, stroke, and even brain damage (Pero et al., 2020). A recent study conducted in the United Kingdom investigating 153 patients, reported COVID-19-related neurological symptoms including acute cerebrovascular (relating to the brain and its blood vessels) incidents and altered mental status (Varatharaj et al., 2020). In a study of 214 patients from Wuhan, China, of the 36.4% of patients demonstrating neurological symptoms, a total of six patients experienced an acute cerebrovascular incident in the form of a stroke (Mao et al., 2020). The high incidence of acute cerebrovascular incidents in COVID-19 patients has been shown to be related to the coagulopathy, marked by elevated D-dimer and fibrinogen (protein compounds circulating in the blood, with important functions in clotting) (Pero et al., 2020). Coagulopathy refers to an impaired ability of the blood to coagulate adequately, resulting in either excessive bleeding or excessive blood clot formation. So in other words, some neurological symptoms or events as a result of COVID-19, are related to problems with blood clotting. Another observational study of 58 COVID-19 patients from Strasbourg, France, reported confusion in 65% of patients, agitation in 49% of patients, and dysexecutive syndrome (emotional, motivational, and cognitive function impairment as a result of frontal lobe brain damage) in 36% of patients (Helms et al., 2020). Some patients with COVID-19 have even reported language deficits in the form of expressive aphasia (partial loss of the ability to produce language and speak), nonverbalism, and akinetic mutism (a rare neurological condition characterised by pathologically reduced body movement, loss of speech, profound apathy, and other symptoms) (Pero et al., 2020). In a study of 417 patients from 12 different European hospitals, 85.6% reported olfactory dysfunction (problems with the sense of smell), of those 20.4% had anosmia (loss of sense of smell), 12.6% phantosmia (olfactory hallucination where you smell scents that aren’t present around you), and 32.4% parosmia (distorted sense of smell), with the remaining having hyposmia (reduced ability to smell and to detect odors)(Lechien et al., 2020). Some other neurological abnormalities reported in COVID-19 patients are summarised in the chart below.
Routes of Nervous System Infection
COVID-19 is also named SARS-CoV-2 for its close relation to SARS-CoV-1, and is known to infect the Central Nervous System (CNS; Pero et al., 2020). COVID-19 infiltrates the CNS via cells expressing angiotensin converting enzyme 2 (ACE2); a receptor that is expressed by neurons and glia in the brainstem and rostral ventrolateral medulla (Pero et al., 2020).
What is interesting is that most samples taken from COVID-19-confirmed patients have not shown COVID-19 in the Cerebrospinal Fluid (CSF; Steardo et al., 2020). Because COVID-19 is not found in the CSF, this suggest that the virus does not enter the CNS through the blood-brain barrier (if you’re interested in the blood brain barrier, see another post I have written about it here). The lack of COVID-19 virus found in the CSF has led to speculation that the neurologic symptoms related to the virus may be caused by a hyperinflammatory state (too much inflammation) caused by massive release of cytokines and chemokines rather than direct viral infiltration into the CNS (Steardo et al., 2020). A hyperinflammatory state refers to uncontrolled immune activation and excessive release of proteins involved in the activity of the immune system. When released, these proteins direct the immune system to do its job, but if they are released in massive amounts, this causes too much inflammation and can overload the system and impair the function of various organs in the body, including the brain. As seen in the chart above, one class of neurological symptoms are a result of inflammation.
The Impacts of COVID-19 on Mental Health
Immediate Impacts
Not only has COVID-19 impacted us physically – the effects of COVID-19 on our mental health and well-being are likely to be profound and long-lasting and will extend beyond those who have been directly affected by the virus (O’Connor et al., 2021). Beyond stresses inherent in the illness itself, stay-at-home orders, quarantine, and isolation, raise concern about how people react individually and collectively. A recent review of psychological impacts in samples of quarantined people and of health care providers may be instructive; it revealed numerous emotional outcomes, including stress, depression, irritability, insomnia, fear, confusion, anger, frustration, and boredom (Pfefferbaum & North, 2020). Specific stressors included greater duration of confinement, having inadequate supplies, difficulty securing medical care and medications, and resulting financial losses (Pfefferbaum & North, 2020).
The pandemic is also exposing the fact that particular vulnerable groups, such as prisoners, patients in psychiatric hospitals or social care homes, people with disabilities, or women experiencing domestic violence or abuse, are at a greater risk of psychological distress because of pre-existing failures in human rights protection (Kola et al., 2021). Older populations are among the most affected by the COVID-19 pandemic in terms of illness severity and mortality. Older populations, among others, are also more likely to suffer psychological impacts due to isolation, which is complicated by pre-existing physical health problems and medical comorbidities, and reduced access to care (Kola et al., 2021). Lockdowns and the diversion of all health-care services to COVID-19, affects people living with existing serious mental illnesses, for whom access to mental health care has been hindered during the pandemic (Kola et al., 2021).

Long-Term Impacts
Without global action specifically in the amelioration of worsening mental health, the COVID-19 pandemic is expected to have worldwide negative impacts on economic and other social determinants of mental health in the long term. The pandemic may result in a potential worldwide suicide increase as a result of increased exposure to known risk factors, such as economic stress, job insecurity and unemployment, social isolation, decreased access to community support, barriers to mental health treatment, and exacerbated physical health problems (Kola et al., 2021). Computational models have combined data from multiple countries, that highlights that job losses due to COVID-19 might result in up to 9570 additional suicides per year worldwide (Kola et al., 2021). Similarly, substance use disorders represent another major cause of mortality that has been seen in previous global recessions (Kola et al., 2021). Lastly, prolonged school closures, which has been prevalent in many countries across the world, are likely to have a profound effect on the mental health of children, adolescents, and young adults (John Joseph et al., 2020). Aside from the important academic benefits of schooling, schools have an essential role in shaping the mental wellbeing of young people by providing socioemotional development through friendship and social support networks, protection from risk-taking behaviours, and delays to early marriage and childbearing (Kola et al., 2021).
Building Resilient Mental Healthcare Systems
While this topic is way too complex to summarise in a single article, we can all agree that the COVID-19 pandemic has affected our health across all contexts of life. One of the emerging conclusions from the pandemic, is that mental healthcare systems worldwide were not equipped to support people adequately. While the effects on mental health and socioemotional wellbeing are widespread in the population, some research shows that vulnerable and socially disadvantaged groups are disproportionately affected, due to lack of support, services, resources etc. This raises a question; which aspects of pandemic management should be made a priority? Perhaps it is time to re-think some health assumptions, and include mental health in the priority healthcare group, and build resilient mental health systems for the future. Various efforts have been, and will continue to be mobilised on these fronts, however here are some actions that can be taken to create better mental health systems:
Integrating mental health services into universal health coverage.
Improving access and coverage of psychosocial interventions.
Eliminating coercion in mental health care.
Integrating mental health interventions into other sectors.
Addressing the mental health of children and young people.
Incorporating technological innovations in mental health services.
*These suggestions are taken from Kola et al. (2021)
Conclusion on Mental Health

The COVID-19 pandemic has disrupted every aspect of life in all countries almost simultaneously and, in this respect, represents a global phenomenon unlike any other in human history. Emerging evidence indicates that the mental health impacts will be large, long-lasting, and greatest in under-resourced contexts and disadvantaged populations (Kola et al., 2021). Unless addressed quickly and urgently, these impacts will contribute to enormous human suffering and social breakdown (Kola et al., 2021). COVID-19 presents a historic opportunity for all countries to reimagine how human society organises itself to recover from these impacts. We need to invest in building mental health systems now but we should also ensure that these investments embrace the diversity of experiences and actions that characterise mental ill health, well beyond the narrow biomedical focus on doctors, diagnoses, and drugs that has dominated mental health policies globally (Kola et al., 2021). We need to not only reimagine mental health care, but also reframe mental health as a common and prioritised aspect of our general health in all countries worldwide.
References
Cullen, W., Gulati, G., & Kelly, B. D. (2020). Mental health in the COVID-19 pandemic. QJM: An International Journal of Medicine, 113(5), 311-312.
Helms, J., Kremer, S., Merdji, H., Clere-Jehl, R., Schenck, M., Kummerlen, C., … & Meziani, F. (2020). Neurologic features in severe SARS-CoV-2 infection. New England Journal of Medicine, 382(23), 2268-2270.
John Joseph, S., Singh Bhandari, S., Ranjitkar, S., & Dutta, S. (2020). School closures and mental health concerns for children and adolescents during the covid-19 pandemic. Psychiatria danubina, 32(2), 309-310.
Lechien, J. R., Chiesa-Estomba, C. M., De Siati, D. R., Horoi, M., Le Bon, S. D., Rodriguez, A., … & Saussez, S. (2020). Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. European Archives of Oto-Rhino-Laryngology, 277(8), 2251-2261.
Mao, L., Jin, H., Wang, M., Hu, Y., Chen, S., He, Q., … & Hu, B. (2020). Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA neurology, 77(6), 683-690.
O’Connor, R. C., Wetherall, K., Cleare, S., McClelland, H., Melson, A. J., Niedzwiedz, C. L., … & Robb, K. A. (2021). Mental health and well-being during the COVID-19 pandemic: longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. The British Journal of Psychiatry, 218(6), 326-333.
Pero, A., Ng, S., & Cai, D. (2020). COVID-19: a perspective from clinical neurology and neuroscience. The Neuroscientist, 26(5-6), 387-391.
Pfefferbaum, B., & North, C. S. (2020). Mental health and the Covid-19 pandemic. New England Journal of Medicine, 383(6), 510-512.
Steardo, L., Steardo Jr, L., Zorec, R., & Verkhratsky, A. (2020). Neuroinfection may contribute to pathophysiology and clinical manifestations of COVID‐19. Acta Physiologica (Oxford, England).
Varatharaj, A., Thomas, N., Ellul, M. A., Davies, N. W., Pollak, T. A., Tenorio, E. L., … & Plant, G. (2020). Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. The Lancet Psychiatry, 7(10), 875-882.
World Health Organization. (2020). Clinical management of COVID-19: interim guidance, 27 May 2020 (No. WHO/2019-nCoV/clinical/2020.5). World Health Organization.
To access the research paper by Drew et al. (2013), follow the following link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3964612/
Latest From Instagram
More from the NeuroBlog

How can Neurofilament light concentrations help in Diagnosis?
Overview In May 2022, I attended a conference in Syndey, Australia. The conference was targeted mainly for psychiatrists and neuropsychiatrists. I was able to attend this lovely conference through my company called Monarch Mental Health Group. On the first day, the conference kicked off by an invited keynote speaker. This speaker was a psychiatrist, and…

Execessive Neural Noise in Developmental Dyslexia?
Overview Developmental dyslexia (reading disabilities/disorders, or decoding-based reading disorder) is a neurodevelopmental disorder with multiple potential underlying genetic, neural, and cognitive factors. Past models have not been very successful at integrating key neural and behavioural features of dyslexia with common neural processes, until Hancock et al. (2017) proposed their dyslexia model. Dyslexia risk genes indicate…

Debunking Popular Neuromyths: Do You Use Your Entire Brain?
It is the summer of 2014 on Earth’s Northern hemisphere and the movie Lucy is hitting theatres. The official promotional posters and movie trailers contain the tagline “The average person uses 10% of their brain capacity. Imagine what she could do with 100%.” Lucy becomes the second most successful debut for a French action film,…
